Frequently Asked Questions (FAQ) and Guide to HIX Usage
What is the Hepatocyte Injury Index (HIX)? Liver injury is well approximated by serum AST and ALT values, especially when the AST and ALT are not changing. However, during periods of AST and ALT change, slow clearance of these biomarkers leads to a decisive lag between the level of actual liver injury, and the level of AST and ALT. This is best seen in simulation here:
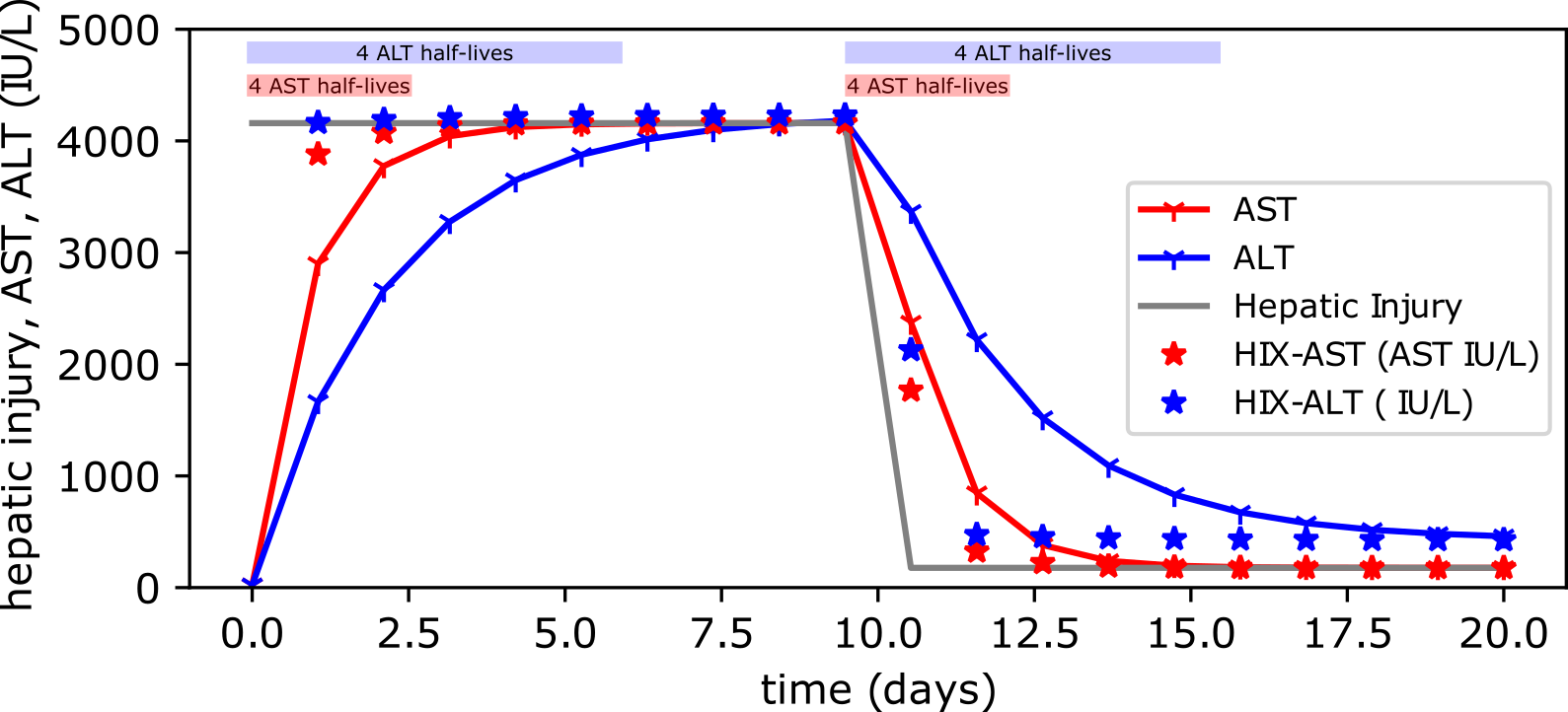
The HIX index (plotted in asterisks) calculates the level that AST or ALT should be during dynamic change and corrects for lag induced by slow clearance.
How do I interpret the HIX? We've constructed the HIX to be interpreted exactly how we (clinicians) currently interpret AST or ALT. Prior to this work, we assumed AST and ALT represented the most up-to-date knowledge of active, worsening, resolving or resolved liver injury. The HIX (aka HIX-ALT) and the HIX-AST directly replace how AST and ALT are interpreted and represent a more up to date view of what the AST or ALT would be if slow clearance is immediately accounted and corrected for.
When would I use the HIX? The HIX is valid for short-interval pairs of measurements of AST and ALT. In simulation, the longest we've examined is up to 2 days between AST or ALT measurements, but in general, the shorter the interval between measurements, the more accurate and informative the HIX will be. Importantly, the HIX does not add value for laboratory testing conducted with >2 days gap, and therefore is likely only useful for hospitalized patients where daily or more frequent laboratory testing is obtained.
Is the HIX making a prediction about liver injury? Yes, and no. The HIX is "predicting" liver injury no more, or less than serial AST or ALT measurements "predict" liver injury. Liver injury may worsen, or improve at any time, and the HIX does not "predict" these events. Rather, one should think of the HIX as taking information that is delayed by 2-5 days (AST and ALT) and updating it to information that is delayed only by the time it takes to obtain two laboratory tests.
How will the HIX change my clinical decision making? Crucially, we have not validated the HIX in prospective studies, and such studies will need to be conducted. That said, here are some examples of the HIX where usual clinical interpretation is obviously altered by application of the HIX.
Case studies 1a and 1b. Use of the HIX in an emergency room markedly alters interpretation of initial acute liver injury (ALI) trajectory.
Case study 1a.
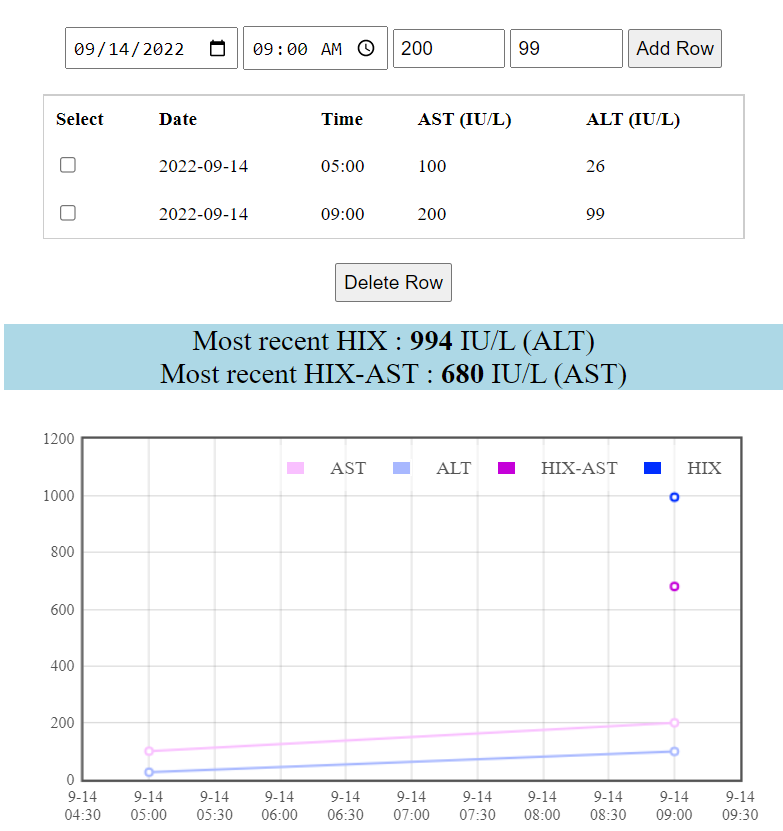
Here, two serum laboratory tests for AST and ALT are taken 4 hours apart in an emergency room patient. The absolute values of AST, and especially ALT are rising, but are not necessarily concerning. Current clinical practice would be to trend enzymes. In contrast, the HIX shows that if we eliminate delay due to slow enzyme clearance, the rise in ALT from 26 to 99 IU/L in 4 hours indicates the equivalent amount of ALT=994, consistent with severe liver injury. Such a patient deserves immediate consideration for a liver biopsy and careful review of medications for possible DILI, rather than watchful waiting.
Case study 1b.
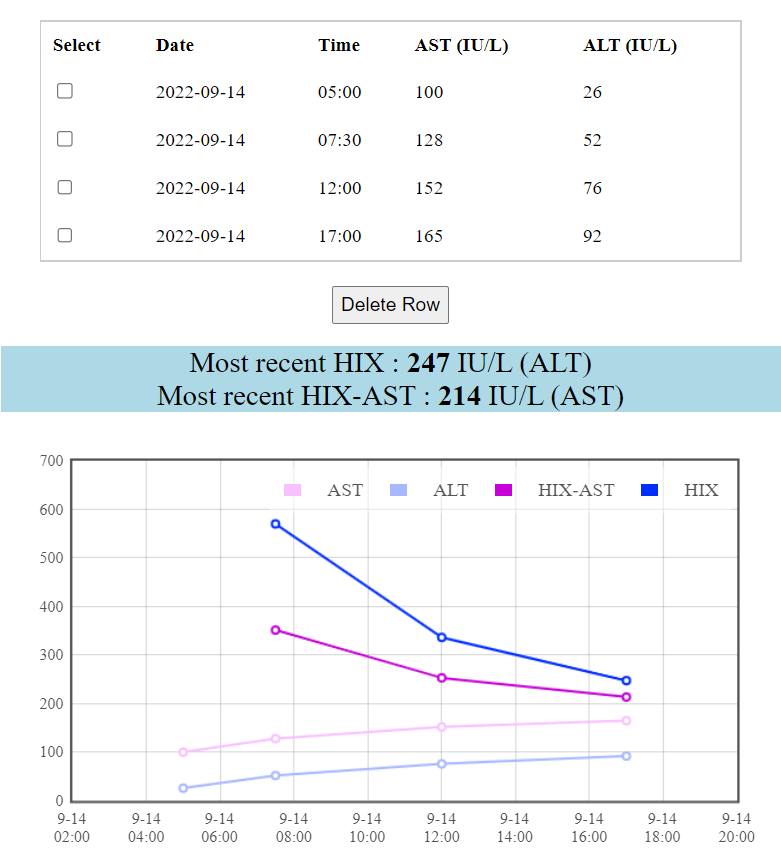
Similar to Case 1a above, we have an emergency room patient with serial laboratory testing that indicates steadily rising transaminases concerning for a worsening acute liver injury. HIX correction conveys a very different story, however, with steady improvement in the degree of liver injury over the course of observation. Here, the interpretation of this patient's trajectory of apparently worsening LFTs is starkly altered by HIX correction which shows improvement; such a patient can likely be discharged with follow up testing.
Case study 2.
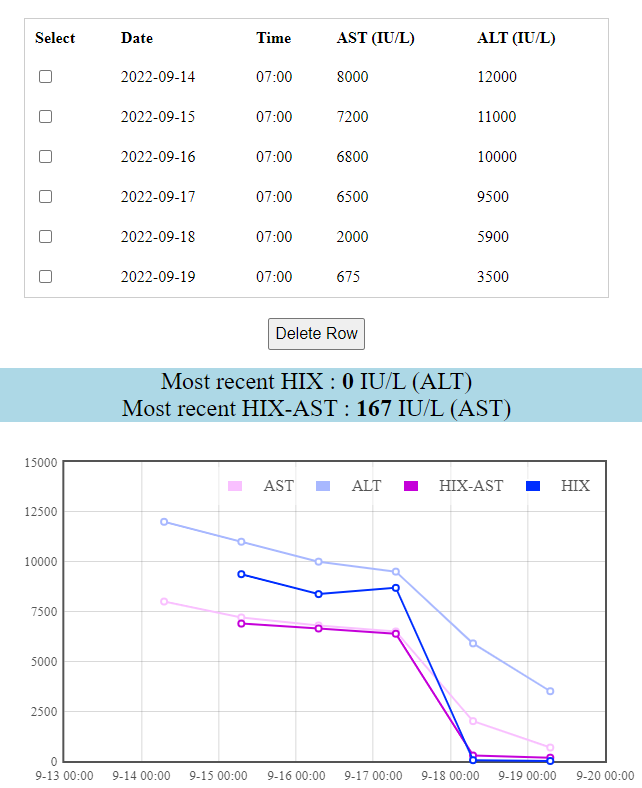
Here we have an admitted patient with daily laboratory testing showing towering LFTs. ALT and AST are improving steadily from Day 0 to Day 3, a sign that perhaps the patient's liver injury is improving and warranting monitoring alone. HIX calculation revises this assessment dramatically, showing that liver injury is unchanged and stable around 8000 ALT IU/L equivalents for day 0 to day 3, indicating ongoing, massive liver injury. On day 4, ALT and AST continue to improve, but the HIX reveals that this improvement actually marks complete resolution of liver injury despite AST=2000 and ALT=5900. By usual practice, we might trend this patient's liver enzymes to baseline, but with the HIX we now realize such a plan is equivalent to watching enzyme being cleared from the blood, rather than resolution of liver injury.